flowchart TB
subgraph inp [Inputs]
direction TB
I1["Images<br/>chest X-ray, fundus,<br/>histopathology, skin photo"]
I2["Text<br/>notes, reports,<br/>social-media posts"]
I3["Signals<br/>ECG, audio,<br/>ultrasound video"]
end
subgraph enc [Encoders]
direction TB
E1["Vision encoder<br/>CLIP / SigLIP,<br/>BiomedCLIP, RETFound"]
E2["Text encoder<br/>GatorTron,<br/>clinical LM"]
E3["Signal encoder"]
end
subgraph fus [Shared multimodal model]
F["Vision-language model<br/>Med-Gemini, BiomedGPT,<br/>general multimodal LLM"]
end
subgraph tsk [Tasks]
direction TB
T1["Classification<br/>screening triage"]
T2["Segmentation<br/>MedSAM"]
T3["Report<br/>generation"]
T4["Visual question<br/>answering"]
end
I1 --> E1
I2 --> E2
I3 --> E3
E1 --> F
E2 --> F
E3 --> F
F --> T1
F --> T2
F --> T3
F --> T4
7 Multimodal Medical AI for Public Health Tasks
The whole art of medicine is in observation.
William Osler, teaching motto
7.1 Learning objectives
By the end of this chapter you should be able to:
- Distinguish vision foundation models (MedSAM, RETFound, BiomedCLIP) from general-purpose multimodal LLMs and choose between them for an imaging task.
- Use clinical AI scribes appropriately, with attention to documentation quality, attestation, and the scribe-clinician verification handoff.
- Apply OCR and table-extraction tools to clinical PDFs and structured-form documents at the scale a research workflow requires.
- Reason about CONSORT-AI and TRIPOD-LLM reporting standards as they apply to multimodal medical AI studies.
- Situate multimodal models within a population-screening program (diabetic retinopathy, tuberculosis, skin and cervical screening) and evaluate screening performance for equity across demographic subgroups and sites.
- Recognize multimodal AI as a tool for digital epidemiology and disease surveillance, and appreciate health misinformation as a multimodal population-health concern.
7.2 Orientation
The arrival of robust multimodal capability changes what can be analyzed in clinical research. Datasets that previously required manual abstraction, chest X-rays, pathology slides, clinical-photograph series, free-text notes, scanned forms, ultrasound video, voice recordings, are now amenable to AI-assisted extraction at scale. The question for the researcher is no longer ‘can we use this kind of data’ but ‘how do we validate the AI-assisted extraction so the downstream analysis is defensible’.
The chapter walks through three practical settings: vision foundation models for biomedical imaging, clinical AI scribes that produce structured documentation from voice recordings of patient encounters, and OCR and table extraction for clinical PDFs. Each has emerged into routine practice in the past two to three years, and each has a characteristic failure mode the researcher must control for.
The unifying theme is that multimodal output, like reasoning-model output, requires a verification regime proportionate to stakes. A radiology report drafted by a multimodal model and signed by a radiologist is different from a research-only annotation; an OCR’d clinical form audited by a research coordinator is different from one fed unchecked into a regression. The researcher designs the validation to match the use.
For the public-health reader, the setting where these models matter most is not the single clinical encounter but the screening program run across a whole population. Diabetic-retinopathy screening from fundus photographs, tuberculosis screening from chest X-rays in high-burden districts, cervical and skin screening from clinical photographs: each is a task where a foundation model can extend expert-level triage to settings that have few experts, and each is a task where a model that performs well on average can still perform poorly for a subgroup that the headline figure conceals. But how well does ‘well on average’ serve the people the program is meant to reach? That question, more than raw accuracy, organizes the population-health parts of this chapter.
The models divide along the modality they read and the task they perform. Figure 7.1 gives that division before we take the classes apart; the point to carry from it is that a single input modality (an image) feeds several distinct tasks (classification, segmentation, report generation, visual question answering), and different model families are strong at different tasks, so ‘which model’ is answered only once ‘which task’ is fixed.
7.3 The researcher’s contribution
Three judgments are not delegable.
(Judgment 1.) Distribution shift in imaging is silent. A model trained on Stanford radiographs may underperform on Brigham radiographs in ways that produce plausible-looking but biased extractions. Different scanners, acquisition protocols, patient populations, and even time-of-day produce subtle shifts that undermine model performance. The researcher designs the validation to detect distribution shift: typically by reserving a substantial site-specific holdout, and treats inter-site variability as a first- order concern.
(Judgment 2.) AI-extracted variables are not interchangeable with manually-extracted variables. A ‘left-ventricular ejection fraction’ field populated by multimodal extraction from echocardiogram reports is not the same as one populated by trained clinical abstractors, even if the marginal distributions match. The error patterns differ, the systematic biases differ, and downstream analyses can be biased in characteristic ways. The researcher documents the extraction method and validates against a manual reference on a sample.
(Judgment 3.) Reporting standards are part of the analysis. CONSORT-AI (Liu et al., 2020) and TRIPOD- LLM (Gallifant et al., 2025) specify what must be reported when AI is involved in a clinical study: training data composition, validation strategy, performance subgroups, deployment context. The researcher follows these standards from the start of the study, not retrofitted at submission. Studies that ignore them are increasingly returned by reviewers and by journals.
7.4 Vision foundation models for biomedical imaging
Three classes of multimodal model handle biomedical imaging differently.
General-purpose multimodal LLMs (multimodal frontier models from major providers) are trained on broad image-text pairs from the web. They handle natural images, diagrams, screenshots, and moderate-quality medical images reasonably. They perform poorly on specialized modalities (histopathology slides, fundus photographs, mammograms) because the training distribution is sparse on these. They are the right starting point for OCR-shaped tasks (extract a table from a clinical PDF), for clinical-photograph description, and for screening triage where rough classification is enough.
Domain-specific foundation models are trained on biomedical image-text pairs and substantially outperform general-purpose models on specialized modalities. Three have become reference points:
MedSAM (Ma et al., 2024) is a foundation model for medical image segmentation. Given an image and a prompt (a bounding box or a text description), it produces a segmentation mask. Useful for organ segmentation, lesion delineation, and tumor measurement. Outperforms general-purpose segmentation on specialized modalities.
RETFound (Zhou et al., 2023) is a foundation model for retinal images, trained on 1.6 million retinal photographs. It produces representations useful for downstream tasks (diabetic retinopathy grading, age-related macular degeneration classification, systemic disease prediction) with small fine-tuning datasets.
BiomedCLIP (S. Zhang et al., 2025) is a vision- language foundation model trained on biomedical image-text pairs from PubMed. It inherits the contrastive image-text training of the general-domain CLIP and SigLIP models, which learn a shared embedding space in which an image and its caption sit close together; BiomedCLIP re-runs that recipe on fifteen million biomedical figure-caption pairs. The practical consequence is zero-shot classification: one can score a fundus photograph against the text prompts ‘referable diabetic retinopathy’ and ‘no referable disease’ without a labeled training set, which is useful when a screening program has images but few labels. BiomedCLIP also serves as an embedding model for biomedical image-text retrieval pipelines. A further step is taken by broader medical multimodal models such as BiomedGPT (K. Zhang et al., 2024) and Med-Gemini (Saab et al., 2024), which add report generation and visual question answering on top of the vision-language backbone.
Specialty-specific clinical models are smaller, deeper-domain models for narrow tasks: a chest-X-ray abnormality classifier, a histopathology grading model, a fundus diabetic-retinopathy grader. These have been common since 2018; the foundation-model approach generally subsumes them but specialty models can still win on narrow benchmarks where they were trained.
The decision rule:
| Task | Recommended starting point |
|---|---|
| Clinical PDF OCR / table extraction | General multimodal LLM |
| Clinical photograph description | General multimodal LLM |
| Image segmentation (medical) | MedSAM |
| Retinal image analysis | RETFound (fine-tuned) |
| Cross-modal retrieval (image ↔︎ text) | BiomedCLIP |
| Specialty radiology / pathology | Specialty model where available, else BiomedCLIP |
The decision rule above is organized by task. Table 7.1 re-organizes the same material around the population-health screening programs this chapter foregrounds, so that a reader who starts from a use case (screen a district for tuberculosis, extend retinopathy screening to primary care) can read across to the modality, task, and representative model family. The column to dwell on is the last one: the screening use case is what fixes the stakes, and therefore the validation regime, for everything to its left.
| Input modality | Task | Representative model family | Public-health screening use case |
|---|---|---|---|
| Fundus photograph | Classification / grading | RETFound (fine-tuned); general multimodal LLM for triage | Diabetic-retinopathy screening in primary care |
| Chest X-ray | Detection / classification | Specialty CXR classifier; BiomedCLIP zero-shot | Tuberculosis screening in high-burden districts |
| Skin photograph | Classification | General multimodal LLM (triage); specialty dermatology model | Skin-lesion triage in teledermatology |
| Cervical image / cytology | Classification | Specialty model; BiomedCLIP | Cervical-cancer screening at scale |
| Any medical image | Segmentation | MedSAM | Lesion and organ measurement for screening follow-up |
| Image + text | Report generation | Med-Gemini, BiomedGPT | Drafting screening reports where readers are scarce |
| Image + text | Visual question answering | BiomedGPT; general multimodal LLM | Triage question answering and patient-facing explanation |
| Clinical or web text | Surveillance / extraction | GatorTron; general LLM | Syndromic surveillance; social-determinant extraction |
A workflow for using a foundation model on a research task:
import torch
from medsam import MedSAM_Inference
model = MedSAM_Inference.load('medsam_vit_b.pth')
# Provide image and bounding box for segmentation
mask = model.segment(
image=ct_slice,
bbox=[120, 80, 380, 320],
)
# Compute volumetric measurement
volume_mm3 = mask.sum() * voxel_volumeThe output (volume_mm3) becomes a study variable. The validation question is: how well does this volume agree with manual segmentation by a radiologist? The answer is task-, site-, and modality-dependent and must be established empirically on a representative subset.
7.5 Population screening at scale and equity
The most consequential public-health use of these models is screening: applying a triage classifier to a whole population so that the scarce expert time is spent on the cases the model flags. A retinal foundation model can grade diabetic retinopathy from fundus photographs captured by a technician in a primary-care clinic; a chest-X-ray classifier can flag probable tuberculosis in a mobile-screening van in a high-burden district; a teledermatology triage model can sort skin photographs into ‘refer’ and ‘reassure’. In each case the model does not replace the specialist but rations access to one, which is precisely the constraint that makes screening at population scale feasible where it previously was not.
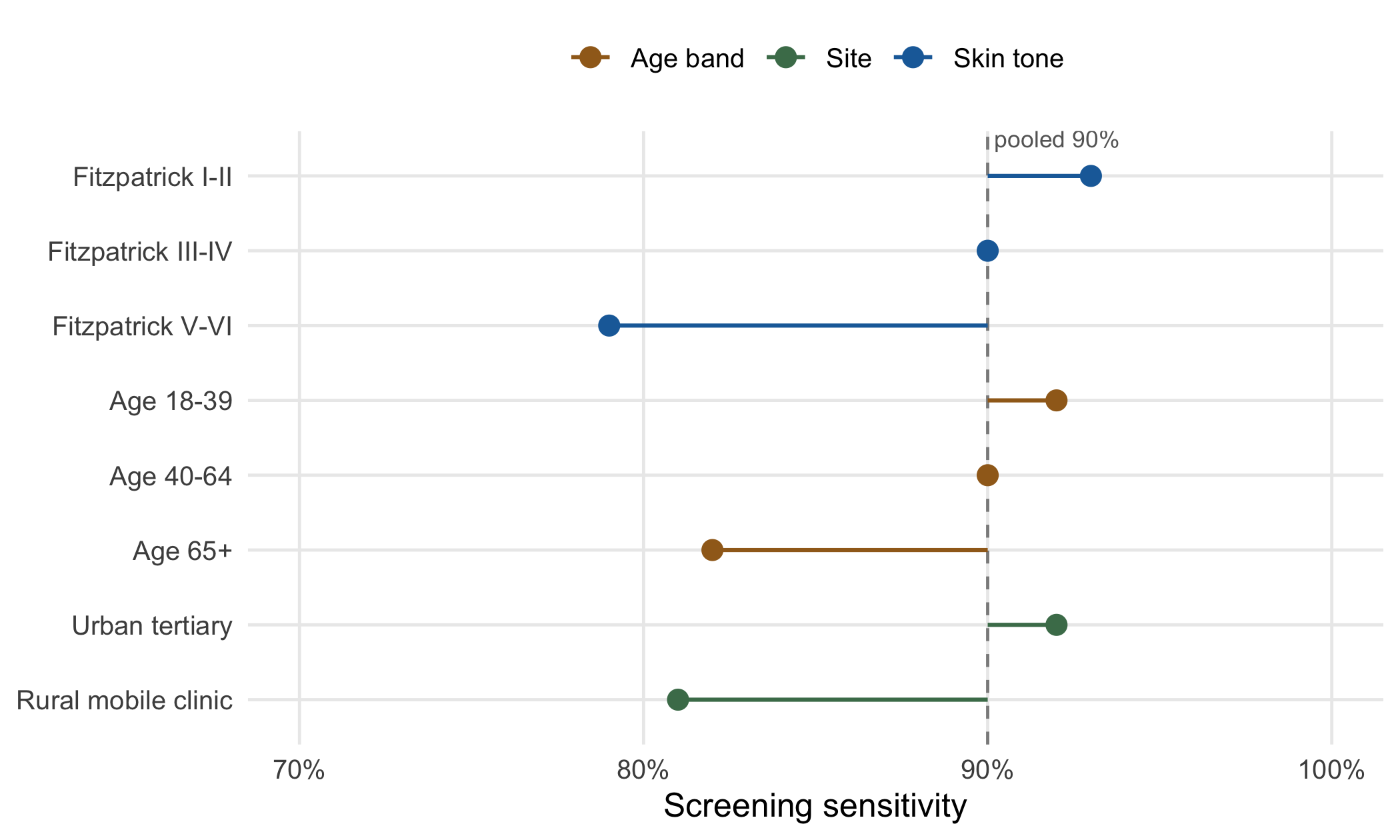
The promise is real, and so is the characteristic failure. A screening model is tuned and reported by its average performance, a single sensitivity and specificity on a held-out set. But a population is not homogeneous, and the training data that produced the model is rarely a representative sample of the population the program will screen. A retinopathy model trained mostly on lighter-skinned patients from tertiary centers may grade darker fundus images less reliably; a model trained on younger cohorts may miss disease in the oldest patients; a model validated at an urban teaching hospital may degrade at a rural mobile clinic with older cameras and different lighting. The average sensitivity can look reassuring while the subgroup sensitivity that actually matters, for the people least well served by the existing system, sits well below it.
Figure 7.2 makes the point with illustrative numbers. What to take from it is not the specific values, which are invented, but the shape: a pooled sensitivity that clears a plausible target hides subgroups (the darkest skin tones, the oldest age band, the rural mobile-clinic site) that fall several points short, and these are frequently the subgroups with the fewest training examples. A screening program evaluated only on the pooled figure would report success while quietly under-serving exactly the populations a public-health program exists to reach.
The remedy is not exotic; it is disaggregated reporting. A screening evaluation should report sensitivity and specificity by the subgroups that matter for the program (skin tone, age band, sex, site, and any axis along which the training data was thin) and should set an acceptance criterion on the worst-performing subgroup, not the average. This is the multimodal-imaging counterpart of the algorithmic-fairness concerns (Obermeyer et al., 2019) raised for tabular risk scores; the modality differs but the discipline is the same. Where a subgroup falls short, the options are familiar: collect more training data for that subgroup, recalibrate the decision threshold per subgroup, or route that subgroup’s cases to human review at a higher rate. What is not defensible is deploying a population-scale screening tool on the strength of a pooled figure alone.
7.6 Digital epidemiology and health misinformation
Multimodal models also reach public health from a second direction, not screening individuals but observing populations. Digital epidemiology, the use of digital traces to monitor health at population scale (Salathé et al., 2012), predates these models by a decade, but multimodal capability widens what counts as a usable trace. Free-text clinical notes, historically locked away from analysis, can be mined for social-determinant signals with clinical language models such as GatorTron (Yang et al., 2022) and purpose-built extractors (Guevara et al., 2024), turning housing instability, food insecurity, and social isolation recorded in prose into structured surveillance variables. Images and video extend the reach further: satellite and street-level imagery for environmental exposures, photographs of vector-breeding sites for arbovirus surveillance, and social-media images alongside their captions for early signals of an emerging outbreak.
The generalist-medical-AI program (Moor et al., 2023) frames this as one capability among many: a model that reads images, text, and signals together can, in principle, support surveillance, triage, and documentation with a single backbone. We should treat that framing with the standing caution of this book. A model good enough to draft a note is not thereby good enough to call an outbreak; the surveillance use has its own validation burden, its own baseline of false alarms, and its own equity problem, because the populations most visible in digital traces are not the populations most at risk.
There is a darker mirror to surveillance. The same multimodal capability that lets us read population signals lets others manufacture them. Health misinformation is increasingly multimodal: a fabricated ‘screening result’ image, a doctored chart, a synthetic testimonial video, or a plausible-looking but invented study figure, any of which can circulate faster than the correction. For the public-health researcher this is not a peripheral concern but a population-health exposure in its own right, and one that multimodal models sit on both sides of: they can help detect coordinated misinformation (by matching recycled images, flagging synthetic artifacts, clustering narratives across posts) and they can lower the cost of producing it. We shall return to the generation side in the chapter on safety and bias; here we note only that a surveillance pipeline reading social media for health signals must be built on the assumption that some of what it reads is manufactured.
7.7 Clinical AI scribes: documentation and attestation
Voice-driven AI scribes have become routine in clinical workflows in 2025–2026. The clinician sees the patient, the scribe records audio (with patient consent), and a multimodal model produces a draft clinical note in the EHR. The clinician reviews and signs.
The technology is mature: products from Abridge, Suki, Nuance DAX, and others integrate with major EHRs and produce structured notes that include HPI, exam, assessment, and plan. From a research perspective, the arrival of AI scribes changes two things:
Note quality is more variable than before. A scribe- generated note approved by a busy clinician may include errors the clinician did not catch. For research that uses clinical notes as input, chart abstraction, phenotype identification, NLP pipelines, the data is noisier than pre-scribe-era notes, often in characteristic ways: medications listed but not prescribed, problems hallucinated from passing mention, exam findings inserted that the clinician did not perform.
Attestation patterns matter for research consent. A scribe-generated note signed by the clinician is the clinician’s attestation. The patient consented to the encounter and to the scribe; the clinician attests to the content. For research that uses the note, the research consent and IRB approval cover the use of the note as documented; the AI-assisted nature of the documentation is usually disclosed in IRB protocols because it affects what the data represents.
The researcher’s role:
Validate phenotype extraction in the AI-scribe era. A phenotyping pipeline trained on pre-2024 notes may underperform on post-2024 notes because the writing style and content patterns have shifted. Re-validation on a recent sample is appropriate when the cohort spans the scribe transition.
Document the AI-assisted documentation. When publishing on a cohort, disclose whether and when AI scribes were used. The disclosure is increasingly an explicit reviewer expectation.
Consider the systematic-bias question. Some patient groups (non-English-speaking, atypical presentations, quiet voices) are systematically under-represented in AI-scribe training and may be under-served by the output. The researcher evaluates whether the cohort includes such groups and whether systematic bias in note quality could affect the analysis.
A clinical AI scribe is in the literature beginning to be evaluated in randomized trials for its effects on clinician workload, note quality, and patient outcomes. (Tu et al., 2025) is the canonical example. The empirical findings: documentation time falls substantially, clinician satisfaction rises, note quality is comparable or slightly better on objective measures. The harder questions, does the scribe miss things the clinician would have caught, does it propagate errors, does it affect patient safety, are still being studied.
7.8 OCR and structured extraction from clinical documents
Clinical research routinely encounters PDFs with structured tables, scanned forms, and other documents where the data is human-readable but not machine- readable. Multimodal LLMs are very good at this task: substantially better than dedicated OCR libraries on typical clinical documents, and have become the default tool for extraction at moderate scale.
A working pattern:
from anthropic import Anthropic
import base64
from pathlib import Path
client = Anthropic()
def extract_table(pdf_page_path: Path) -> dict:
image_data = base64.standard_b64encode(
pdf_page_path.read_bytes()
).decode('utf-8')
response = client.messages.create(
model=os.environ.get('LLM_MODEL', 'claude-opus-4-7'),
max_tokens=4000,
messages=[{
'role': 'user',
'content': [
{'type': 'image', 'source': {
'type': 'base64',
'media_type': 'image/png',
'data': image_data,
}},
{'type': 'text', 'text':
'Extract the laboratory values from '
'this clinical document as JSON with '
'keys: test_name, value, units, '
'reference_range, date_collected. '
'Return ONLY valid JSON.'},
],
}],
)
return parse_json(response.content[0].text)The extraction quality is high but not perfect. Three patterns of validation:
Schema validation. The output is JSON; check it parses and has the expected keys. Failures here are malformed output, easily caught.
Sample manual review. For a sample of extractions (5–10% is typical), have a research coordinator review the original document against the extracted output. Log discrepancies; address systematic ones with prompt changes.
Distribution checks. For continuous variables, the distribution of extracted values should look like the expected clinical distribution (heart rate centerd near 75, not near 750 because of unit confusion). Outliers flag both genuine outliers and extraction errors; investigate either way.
A nuance: multimodal extraction from PDFs with native text sometimes underperforms text-only extraction from the same PDF. If the PDF has selectable text, use PyPDF or pdfplumber to extract text, then ask the model to parse the text, faster, cheaper, and often more accurate than image-based extraction. Reserve image- based extraction for scanned forms, handwritten notes, and documents where layout matters more than text.
7.9 Worked example: a chest-X-ray cohort study
A pulmonology team wants to study trajectories of pulmonary fibrosis in a cohort of 800 patients with serial chest X-rays. Each patient has 3–6 X-rays over 2–10 years; the goal is to extract a fibrosis severity score from each X-ray for longitudinal modeling.
Step 1: define the variable. The team specifies a 0–4 fibrosis severity score, with anchored definitions for each level matching the radiologist scoring used in two prior published cohorts.
Step 2: choose the extraction approach. The team considers three options:
- Manual scoring by a radiologist: gold standard, ~5 minutes per image, ~$10/image, total ~$30,000 across 3,000 images.
- Multimodal LLM with the score definitions as part of the prompt: $0.05 per image, total $150, fast.
- Specialty CXR model fine-tuned for fibrosis scoring: requires a labeled training set; not available.
The team chooses a hybrid: multimodal LLM for the bulk of the cohort, plus radiologist scoring on a 200-image validation subset.
Step 3: build and validate the extraction pipeline. The validation subset shows the multimodal LLM has a weighted Cohen’s kappa of 0.71 against the radiologist, moderate-substantial agreement. The agreement is weaker for severe fibrosis (kappa 0.61 for score 3-4) than for mild (kappa 0.78 for score 0-1). The team documents the validation and decides:
- Use the LLM scores for all 3,000 images.
- Include kappa = 0.71 in the methods.
- Plan a sensitivity analysis where the longitudinal model is refit using only the 200 radiologist-scored images, to confirm robustness.
Step 4: extract. The pipeline runs in about 4 hours, costs about $150, and produces fibrosis scores for all 3,000 images.
Step 5: longitudinal model. A linear mixed model with a fibrosis-score outcome, time as the primary predictor, and patient-level random intercepts and slopes. The fixed-effect coefficient on time is the quantity of interest.
Step 6: sensitivity analysis. Refit the model on the 200 radiologist-scored images. The time coefficient is within 6% of the LLM-score-based estimate; the confidence intervals overlap. The conclusion that fibrosis progresses at roughly the published rate is robust.
Step 7: report. The methods section discloses:
- The fibrosis scoring rubric.
- The multimodal LLM extraction with kappa against radiologist reference.
- The sensitivity analysis results.
- The CONSORT-AI / TRIPOD-LLM checklist as a supplementary file.
The total study cost is roughly $30,000 less than the all-manual approach, the sensitivity analysis confirms the substantive conclusion, and the disclosure documents the AI-assisted nature of the extraction honestly.
7.10 Collaborating with an LLM on multimodal medical AI
Three prompt patterns illustrate working with multimodal models on biomedical tasks.
Prompt 1: ‘Extract this structured data from the attached clinical document.’ Provide the document (PDF, image) and the schema.
What to watch for. Multimodal extraction is sensitive to prompt specificity. ‘Extract the lab values’ will produce variable output; ‘Extract lab values matching this JSON schema with the following fields…’ produces consistent output. Specify units, expected types, and what to do when values are absent.
Verification. Schema-validate the output. Spot-check a sample against the source. Investigate any systematic discrepancies.
Prompt 2: ‘Describe the abnormalities in this medical image.’ Provide the image with relevant context (study type, clinical question).
What to watch for. General multimodal LLMs produce plausible-sounding image descriptions that may include findings that are not present (especially when prompted in a way that suggests there should be findings). They can also miss subtle findings that specialty models catch. Use only as a triage or screening tool, never as a diagnostic substitute.
Verification. Compare against radiologist reads on a sample. For research use, treat the LLM description as a preliminary annotation that requires expert review before becoming a study variable.
Prompt 3: ‘Audit this AI-scribe-generated note for accuracy.’ Provide the note and the audio transcript.
What to watch for. The LLM can flag obvious errors (medications listed but not discussed in transcript, findings hallucinated from passing mention) but may miss subtle ones (the clinician’s tone implying disagreement that the transcript flattens). The audit catches gross errors; expert review catches the rest.
Verification. For high-stakes notes (oncology, surgery), human audit. For routine notes, LLM audit with random sampling for human review.
The meta-pattern: multimodal models accelerate extraction but do not replace expert review for high- stakes decisions. Use them where the speed-up is substantial and the validation can be made rigorous; avoid them where the cost of a missed finding is high and validation cannot keep pace.
7.11 Principle in use
Three habits define defensible work in this area:
Validate against expert reference on a sample. Every multimodal extraction pipeline that produces a study variable has a validated agreement statistic against an expert-derived reference on a representative subset. Without it, the study cannot answer the question ‘how much do extraction errors bias the result’.
Plan distribution-shift checks across sites. When a cohort spans multiple imaging sites or scanner makes, the extraction performance can vary substantially. Build site-stratified validation into the protocol.
Disclose AI-assisted extraction in methods. The disclosure includes the model, the validation approach, the agreement statistic, and any sensitivity analyses comparing AI-extracted to expert-extracted variables.
7.12 Exercises
Take a multimodal task in your workflow (a PDF, an image, a structured form) and extract data with a multimodal LLM. Validate against manual extraction on 20 records. Compute agreement statistics and document the failure modes.
Run the same image through a general-purpose multimodal LLM and a specialty model (e.g., MedSAM for segmentation, RETFound for retinal). Compare the outputs.
For a cohort study using AI-extracted variables, plan a sensitivity analysis: what specific assumption about AI accuracy could change the substantive conclusion? Implement and report.
Compare LLM extraction from a PDF using image-based prompting versus text-extracted prompting (where text is extractable). Document the relative accuracy and cost.
Audit an AI-scribe-generated note against the underlying audio (or pre-AI-era equivalent documentation). Identify the failure modes and their frequency.
7.13 Further reading
- Ma et al. (2024), Segment Anything in Medical Images. The MedSAM reference.
- Zhou et al. (2023), A foundation model for generalizable disease detection from retinal images. The RETFound reference.
- S. Zhang et al. (2025), BiomedCLIP: a multimodal biomedical foundation model pretrained from fifteen million scientific image-text pairs. The BiomedCLIP reference.
- Moor et al. (2023), Foundation models for generalist medical artificial intelligence. The framing of a single multimodal backbone spanning imaging, text, and signals across tasks.
- Saab et al. (2024), Capabilities of Gemini models in medicine. A medical multimodal model spanning imaging, report generation, and question answering.
- Salathé et al. (2012), Digital epidemiology. The founding statement of using digital traces for population-scale disease surveillance.
- Obermeyer et al. (2019), Dissecting racial bias in an algorithm used to manage the health of populations. The reference case for subgroup performance disparity in a deployed health algorithm.
- Cruz Rivera et al. (2020), Guidelines for clinical trial protocols for interventions involving artificial intelligence: the SPIRIT-AI extension. The reference for protocol-stage AI reporting.
- Liu et al. (2020), Reporting guidelines for clinical trial reports for interventions involving artificial intelligence: the CONSORT-AI extension. The reference for trial-report AI reporting.
- Gallifant et al. (2025), TRIPOD-LLM. The reporting guidance specifically for LLM-based prediction models in clinical research.